Rebecca N. Revell, BSN, RN, CCDS, and Trent M. Bourgeois | Presented at HRS 2026 Health Equity Abstracts Award Session
Remote monitoring is standard of care in CIED management, but its benefit depends on continuous transmitter connectivity. When devices go offline, automated outreach calls prompt reconnection. Most platforms now offer language-matched outreach. A new analysis across more than 100 clinics asks whether that accommodation is sufficient.
THE STUDY
Over 12 months (October 2024–October 2025), Revell and Bourgeois analyzed automated outreach calls for disconnected transmitters across a large remote monitoring platform. Pre-recorded calls were delivered in English or Spanish based on documented language preference using identical scripts. The cohort included 50,757 English-speaking patients (143,431 calls) and 183 Spanish-speaking patients (376 calls). Primary outcomes were call success (calls resulting in a transmission) and patient success (patients who transmitted after receiving a call), [RL1] compared using chi-square tests.
THE FINDINGS
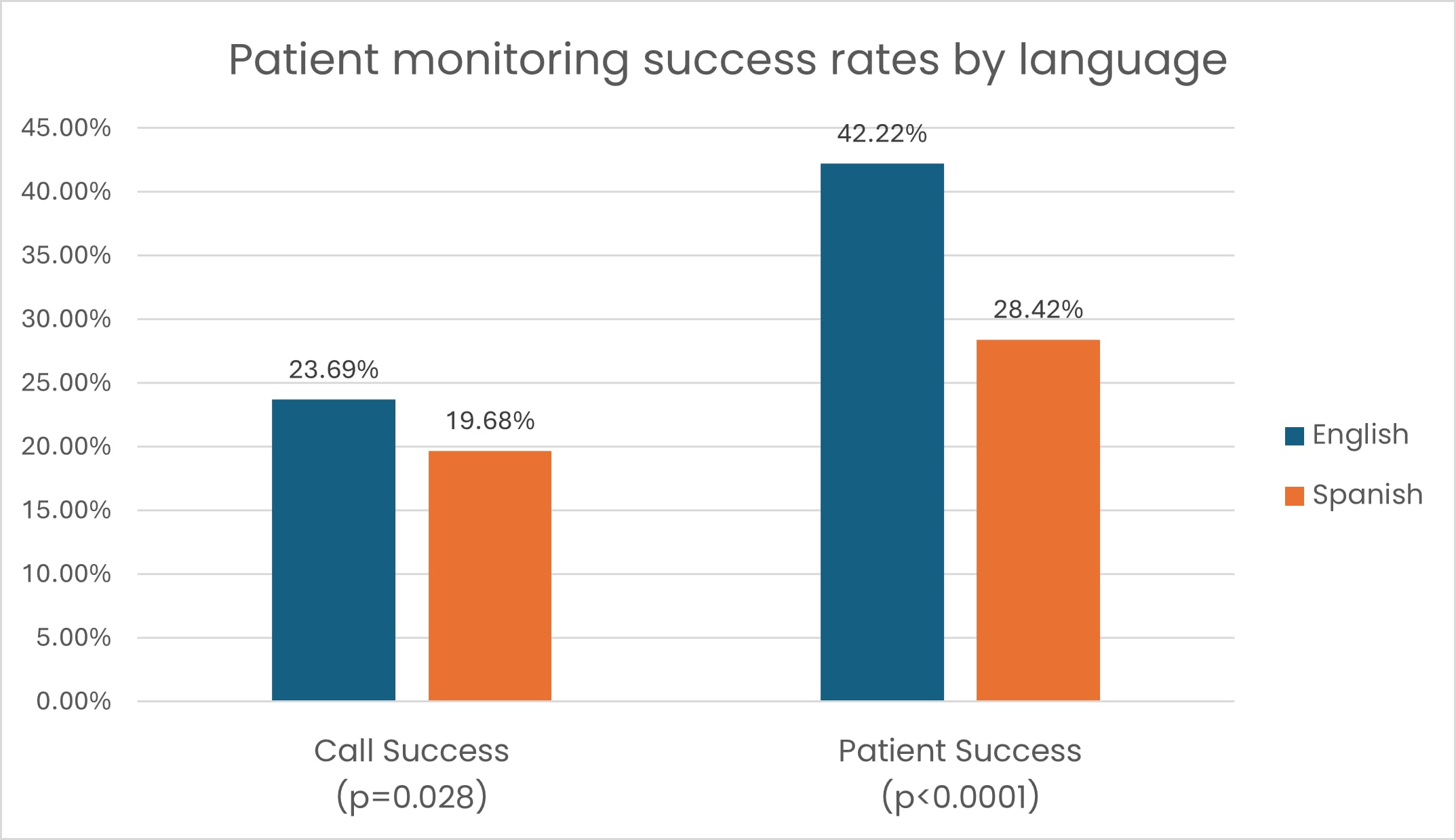
Despite language-matched outreach, Spanish-speaking patients demonstrated significantly lower outcomes at both endpoints:
- Call success: 19.68% versus 23.69% for English-speaking patients (p = 0.028)
- Patient success: 28.42% versus 42.22% (p < 0.0001)
Spanish-speaking patients were 33% less likely to reconnect their devices. The disparity extended beyond disconnection calls: across all call types, call success was 24.96% versus 33.49% and patient success 36.89% versus 54.07% (both p < 0.0001), suggesting a systemic rather than situational pattern.

BEYOND TRANSLATION
The study was not designed to establish causality, and the Spanish-speaking cohort was substantially smaller than the comparison group. What the data cannot resolve is whether the gap reflects the call itself or whether language preference proxies for deeper structural determinants: health literacy, socioeconomic barriers, technological access, or cultural norms around automated communication. The findings do not answer the "why" — they establish that the disparity is real, reproducible, and clinically meaningful, and that causality research is the necessary next step.
Three Key Takeaways
1. Language-matched outreach is necessary but not sufficient. Disparities persisted despite identical technology and scripts. The determinants of inequity likely lie in health literacy, system trust, or communication modality — factors a standardized automated call cannot address.
2. The disparity is systemic, not situational. The gap was consistent across all call types, suggesting the automated outreach model itself may be structurally misaligned with the needs of this population.
3. Closing the outcome gap requires closing the evidence gap. Prospective studies disaggregating outcomes by language preference, health literacy, socioeconomic status, and outreach modality are needed before targeted interventions can be designed with confidence.
Published in Heart Rhythm Journal. View the full publication.
WATCH THE VIDEO
Rebecca Revell speaks about the study findings.
Share in



